Screening mammography remains the only clinically proven imaging modality shown to reduce mortality from breast cancer.1 Current recommendations on when breast cancer screening should commence in women with average risk varies between guidelines. The American Cancer Society (ACS) as well as the joint position of the American College of Radiology (ACR) and the Society of Breast Imaging support annual screening mammography starting at age 40 years.2 The US Preventative Services Task Force and the International Agency for Research on Cancer (IARC) recommend that screening begin at age 50 years and could be biennial.3,4 They acknowledge some data demonstrating screening benefits in women ages 40 to 49 years, but find these data to be limited or insufficient in quality, and therefore recommend screening in women younger than age 40 years to be performed on an individualized basis. While screening mammography has improved the detection of breast cancer, it still has several limitations as a screening test in young women, women with dense breasts, and in BRCA mutation carriers, where mammography sensitivity can be lower. In addition, interval breast cancers still occur in 10% to 35% of women despite adequate screening.5
Multiple studies have evaluated screening breast magnetic resonance imaging (MRI) in women at the highest risk of breast cancer in an effort to address some of these mammographic limitations. A recent meta-analysis reviewed the 11 prospective, nonrandomized, MRI screening studies in high-risk women, finding that the sensitivity of MRI exceeds that of mammography (75% vs 32%, respectively), with the combination of mammography and MRI demonstrating the highest sensitivity, at 84%.6
It is important to acknowledge the difference in the mammographic and MRI screening populations. MRI screening studies included only women with a significant family history or proven genetic mutation, producing an inherent, albeit purposeful, selection bias. This is meaningful in interpretation, but caution is needed for the extrapolation of the MRI screening data to the average-risk screening population. Currently, the lower specificity of MRI compared with mammography, even in the highest-risk populations, results in limitations that include higher call-back rates, increased biopsy rates, increased costs, and the need for intravenous (IV) contrast.7 Furthermore, unlike the nationally accepted mammography standards set by the Mammography Quality Standards Act and Program (MQSA), MRI guidelines beyond minimum imaging requirements are lacking, which allows for variations in institutional protocols regarding image acquisition and sequences. These variations may affect image interpretation or transfer of patient information between institutions and lead to additional imaging recommendations.
Breast Cancer Screening Guidelines
In an effort to streamline MRI screening, ACS published the first set of screening-MRI guidelines in 2007.8 These guidelines support MRI screening in addition to mammography in women at the highest risk for breast cancer, including women or the first-degree relatives of women with BRCA, p53, or PTEN mutations, women with a lifetime risk of breast cancer greater than 20%,9,10 and women with a history of therapeutic chest radiation before age 30. Recent population-based data have shown a rise in the use of screening MRI related to these guidelines; screening MRI accounts for nearly 30% of all MRIs performed.11,12 Little controversy remains on the effectiveness of screening breast MRI, with contemporary data continuing to demonstrate an incremental cancer yield of 15 to 18 cancers per 1000 women screened found by MRI alone after negative mammography in these highest-risk populations.13
The current National Cancer Center Network (NCCN) guidelines14 endorse the ACS recommendations and further address when screening should start and end. For BRCA mutation carriers, screening should begin with MRI annually from ages 25 to 29 years, then annually with mammography and MRI from ages 30 to 74 years, and individualized screening strategies after age 74. Women with a lifetime risk greater than 20% by a family history–specific model should begin annual mammography and MRI at age 30. The guidelines allow for physician discretion as to whether the mammogram and MRI should be performed together or at 6-month staggered intervals. Limited studies have evaluated this question of timing. The MRI-screening trials performed mammogram and MRI at the same time point annually and found an interval cancer rate of approximately 3%.
Le-Petross et al15 studied 73 BRCA1/2 mutation carriers, alternating mammogram and MRI every 6 months. With a median follow-up of 2 years, they found 12 cancers detected by MRI that were not visualized on the mammogram 6 months prior. They concluded that further prospective study is warranted, questioning whether the already low interval cancer detection rate could be further reduced.
Risk Assessment
The debate surrounding screening MRI focuses on resource allocation, on the ability to adequately quantify risk by identifying eligible patients with and without a family history of breast cancer, and on emerging data on lifetime risks of breast cancer primarily in the group classified by ACS as having insufficient evidence to support screening MRI. Clearly, an educational opportunity exists to improve patient and clinician knowledge regarding the role of MRI in breast cancer screening. Wernli et al11 recently reviewed 5 national Breast Cancer Surveillance Consortium registries and documented that less than 5% of women with a lifetime risk of breast cancer greater than 20% are being screened, and that among the MRI-screened population, only 29% had a lifetime risk greater than 20%.
The ability of clinicians to consistently and reliably quantify an individual patient’s cancer risk remains challenging and may explain the discordance found in the Wernli study between estimated risk and use of MRI. The existing ACS and NCCN guidelines do not recommend one risk assessment model over another, but rather suggest using a model that is heavily reliant on family history, such as the BRCAPRO, Tyrer-Cuzick, or Claus models. Using the Gail model is discouraged because it assesses only limited family history. Unfortunately, because the models rely on different input variables, and because they were derived from different populations, it is likely that the models will disagree on exact risk. In fact, Ozanne et al16 compared risk assessment values attained by the Claus, Tyrer-Cuzick, and BRCAPRO models in a community-based hospital setting of 5894 women undergoing screening mammography, of whom 5.8% were eligible for MRI. They found significant variation in the number of women identified by each model who met the 20% threshold, and that the models collectively agreed on patient risk greater than 20% in only 18 of 342 eligible high-risk patients. Improving and individualizing patient risk assessment remains an area of active research.
While these risk-assessment models remain the most highly discussed standardized methods to define cancer risk, the question of enhanced surveillance with MRI in addition to mammography remains for those women with high-risk breast lesions classified as having insufficient evidence according to ACS. Specifically, are there women without a family history of breast cancer, a high-risk inherited mutation, or a history of chest-wall irradiation at sufficient risk to warrant MRI screening for whom the existing models may underestimate risk? Current data with respect to the role of screening MRI in women with high-risk breast lesions or clinical situations considered by ACS and NCCN to have insufficient evidence for routine screening MRI are reviewed next.
Two studies to date have evaluated the role of screening MRI in the setting of atypical ductal hyperplasia (ADH). Port et al17 found no additional cancers detected by MRI alone in 47 screened patients, while Schwartz et al18 found only 2 additional cancers in 131 women. In addition, they reported a 24% need for second-look imaging and a positive predictive value (PPV) of biopsy of 20%, highlighting the complexities of additional MRI screening. Both studies concluded that MRI is not indicated in the setting of ADH. Despite these negative studies on the additive value of screening MRI in the ADH population, emerging data suggest that women with atypical ductal or lobular hyperplasia may in fact have a much higher lifetime risk of breast cancer than previously estimated, and therefore may benefit from screening MRI.
Hartmann and colleagues19 followed 698 women with ADH or atypical lobular hyperplasia (ALH) diagnosed by breast biopsy between 1967 and 2001. With a median follow-up of 25 years, they demonstrated a cumulative risk of breast cancer of 29%, with more than 80% of the breast cancers being invasive. Further, no difference in breast cancer risk existed between those women with ADH or ALH. These data mirror those of the Nashville breast cohort.19,20 Interestingly, the number of foci as 1, 2, or more than 3 further stratifies risk, with more foci of ADH conferring higher risk for future breast cancer. Although these studies did not specifically evaluate MRI effectiveness in women with ADH or ALH, this unique, robust dataset argues in favor of screening MRI in this population based on increased lifetime risk.
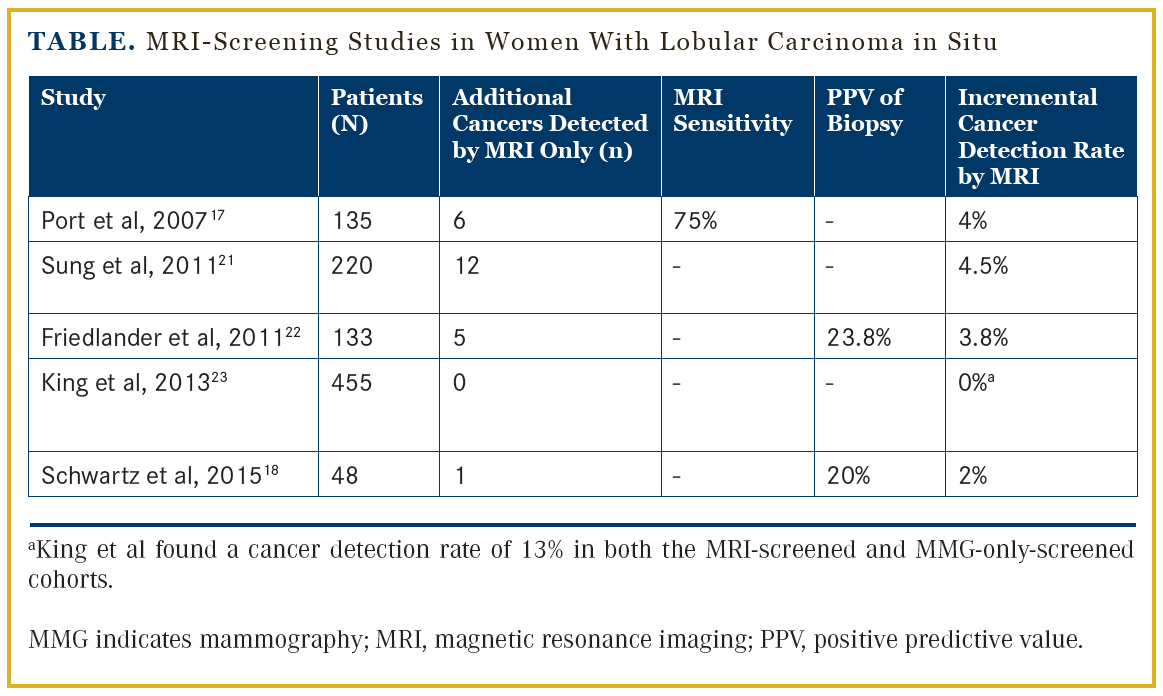
MRI screening for lobular carcinoma in situ (LCIS) also has been studied. Of the 5 available studies, the collective incremental cancer detection rate for MRI screening ranged from 0% to 4%17,18,21-23 (Table). The largest study by King et al23 followed 776 patients diagnosed with MRI, of whom 455 were screened with MRI at the discretion of the treating physician. With a median follow-up of 58 months and a median of 3 MRIs per patient, no difference in crude cancer detection rate was demonstrated, finding cancer in 13% of those screened with MRI and in 13% of those screened with conventional imaging. Further, the study demonstrated that patients followed with MRI were 3 times as likely to have an additional needle biopsy (P <.0001). Finally, MRI screening was not associated with finding smaller tumors or an earlier stage at diagnosis. The authors concluded that insufficient evidence exists to support MRI screening in patients with a diagnosis of LCIS.23
Breast density is currently a screening challenge. With increasing legislation regarding breast density reporting, there is significant interest in screening modalities for these patients. However, to date, consensus opinion on the specific modality recommended or proven to be most effective is lacking. About 50% of women are categorized as having heterogeneously (D3) or extremely dense (D4) breast tissue. Magnetic resonance imaging screening studies thus far have screened women at high risk for breast cancer regardless of breast density. The ACRIN 6666 trial7 evaluated MRI in women at elevated risk for breast cancer after negative mammogram and ultrasound studies. The MRIs did find an additional 14.7 cancers per 1000 women screened.
However, screening MRI in this population was associated with a high false-positive rate, increased biopsies, and a PPV for biopsy of only 18%.
Again, because ACRIN 6666 and other MRI screening studies were performed on women with elevated breast cancer risk regardless of breast density, the benefit of MRI screening in women with dense breast tissue and average breast cancer risk is unclear. Based on the high false-positive rates, cost, and need for IV contrast, the ACR Appropriateness Criteria24 and ACS recommend screening MRI only in women at high risk for breast cancer. Specifically, ACS reaffirms that insufficient criteria remain for MRI screening for patients with dense breast parenchyma without other risk factors.8 Further, no current risk-assessment models incorporate breast density as an input variable. As a result, there is no consensus on whether supplemental screening should be pursued in these patients.
Personal/Family History of Breast Cancer
The ACS also has categorized a personal history of breast cancer as insufficient evidence to support routine use of screening breast MRI after cancer treatment. Emerging data challenge this paradigm, but to date are not widely accepted. Brennan et al25 reviewed 144 women with a personal history of breast cancer without a family history of breast cancer. They reported a 7% incremental cancer detection rate in the ipsilateral or contralateral breast with MRI, resulting in a PPV of biopsy of 39%. Schacht et al26 expanded upon these findings, evaluating 97 women with both a personal and family history of breast cancer. All women had mammogram and MRI. Screening MRI detected cancer in 6 of 92 women (6.5%; ipsilateral or contralateral breast) for a relative risk of 3.04 (95% CI, 1.05-8.86), where family history of breast cancer was used as the referent value. A personal history of breast cancer alone carried a relative risk of only 1.42 (95% CI, 0.48-4.17). They concluded that women with a personal and family history of breast cancer should be screened with MRI and the highest degree of scrutiny.26 Together, these data are hypothesis-generating, but should be interpreted with caution because they were retrospectively collected, did not further delineate lifetime risks of breast cancer in the MRI-screened population having both personal and family history of breast cancer, and likely represent a highly selected population, limiting their generalizability.
Finally, in this era of personalized medicine and the rapid expansion and adoption of genetic panel testing, clinicians will be faced with genetic mutations and variants of lesser known or studied genes. Careful attention to a patient’s family pedigree may help determine the need for enhanced screening. As data accumulate on these new mutations, they can be reclassified. For example, it is now clear that germline mutations in PALB2 significantly increase the risk of breast cancer by age 70. Carriers without a family history of breast cancer have a 33% risk, and those with 2 or more first-degree relatives have a 58% risk of breast cancer by age 50.27 Clearly, these women meet lifetime breast cancer risk criteria for screening MRI.
Advancements in Screening
While the discussions continue regarding the role of MRI in specific clinical situations, clinicians must recognize that advances are being made in the technology of image acquisition and MRI access, as well. Kuhl et al28 recently published prospective, observational, reader study data obtained from 443 women with mild-to-moderate breast cancer risk who had completed 606 rapid (3-minute) screening breast MRIs.28 They found comparable performance results between the rapid and the standard 21-minute MRI screen for breast cancer. Specifically, rapid MRI found 11 cancers after negative mammogram, of which 7 were invasive and 4 were ductal carcinoma in situ (DCIS), for an additional cancer yield of 18.2 per 1000. Furthermore, this abbreviated-protocol MRI required less than 30 seconds to read a complete exam.28 These advancements eliminate several of the barriers that currently limit MRI screening to women at highest risk by providing an option that is quick, sensitive, and far more affordable. Additional trials are needed to confirm these promising results, but confirmation could alter future screening recommendations.
In summary, the value of screening MRI is in the increased detection of breast cancer. Screening MRI is recommended for women at highest risk of breast cancer. Clinicians must understand the limitations and value of risk-prediction models, as this may influence patient eligibility for screening MRI. Some women with atypia or a personal history of breast cancer may benefit from MRI screening, but overall, a one-size-fits-all screening model does not work. As with treatment paradigms, screening must be individualized, and models and guidelines may not accurately capture all women who may benefit from MRI screening. It remains difficult to assess the long-term outcomes and benefits of MRI because the MRI screening trials were not powered to evaluate survival.6 Furthermore, research is needed to assess the impact of anxiety and additional procedures resulting from the variable specificity of MRI on patient quality of life and on the biologic significance of MRI-only-detected cancers.
Affiliations: Sarah A. McLaughlin, MD, is associate professor of Surgery, Mayo Clinic, Jacksonville, FL.
Disclosure: Dr McLaughlin reports no relevant financial conflicts of interest to disclose.
Address correspondence to: Sarah A. McLaughlin, MD, Department of Surgery, Mayo Clinic, 4500 San Pablo Rd, Jacksonville, FL 32224. Fax: 904-953-7368; email: Mclaughlin. [email protected].
References
- Bleyer A, Welch HG. Effect of three decades of screening mammography on breast-cancer incidence. N Engl J Med. 2012;367(21):1998-2005.
- Rebner M. SBI Statement on United States Preventive Services Task Force Draft Research Plan for Breast Cancer. November 25, 2013. http://www.sbi-online.org/Portals/0/Position%20 Statements/2013/SBI%20Response%20to%20USPSTF%20 Draft%20Review%20Process%20-%2011-13.pdf. Accessed July 7, 2015.
- Screening for breast cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;151(10):716-726, W-236.
- Lauby-Secretan B, Scoccianti C, Loomis D, et al. Breast-cancer screening--viewpoint of the IARC Working Group. N Engl J Med. 2015;372(24):2353-2358.
- Hofvind S, Skaane P, Vitak B, et al. Influence of review design on percentages of missed interval breast cancers: retrospective study of interval cancers in a population-based screening program. Radiology. 2005;237(2):437-443.
- Warner E, Messersmith H, Causer P, et al. Systematic review: using magnetic resonance imaging to screen women at high risk for breast cancer. Ann Intern Med. 2008 6;148(9):671-679.
- Berg WA, Zhang Z, Lehrer D, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA. 2012 4;307(13):1394-1404.
- Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. Cancer. 2007;57(2):75-89.
- Claus EB, Risch N, Thompson WD. Autosomal dominant inheritance of early-onset breast cancer. Implications for risk prediction. Cancer. 1994;73(3):643-651.
- Antoniou AC, Pharoah PP, Smith P, Easton DF. The BOADICEA model of genetic susceptibility to breast and ovarian cancer. Br J Cancer. 2004;91(8):1580-1590.
- Wernli KJ, DeMartini WB, Ichikawa L, et al. Patterns of breast magnetic resonance imaging use in community practice. JAMA Intern Med. 2014;174(1):125-132.
- Stout NK, Nekhlyudov L, Li L, et al. Rapid increase in breast magnetic resonance imaging use: trends from 2000 to 2011. JAMA Intern Med. 2014;174(1):114-121.
- Chiarelli AM, Prummel MV, Muradali D, et al. Effectiveness of screening with annual magnetic resonance imaging and mammography: results of the initial screen from the Ontario high risk breast screening program. J Clin Oncol. 2014;32(21):2224-2230.
- National Comprehenisve Cancer Network. NCCN guidelines for breast cancer screening and diagnosis. www.nccn.org. Accessed July 7 , 2015.
- Le-Petross HT, Whitman GJ, Atchley DP, et al. Effectiveness of alternating mammography and magnetic resonance imaging for screening women with deleterious BRCA mutations at high risk of breast cancer. Cancer. 2011;117(17):3900-3907.
- Ozanne EM, Drohan B, Bosinoff P, et al. Which risk model to use? Clinical implications of the ACS MRI screening guidelines. Cancer Epidemiol Biomarkers Prev. 2013;22(1):146-149.
- Port ER, Park A, Borgen PI, et al. Results of MRI screening for breast cancer in high-risk patients with LCIS and atypical hyperplasia. Ann Surg Oncol. 2007;14(3):1051-1057.
- Schwartz T, Cyr A, Margenthaler J. Screening breast magnetic resonance imaging in women with atypia or lobular carcinoma in situ. J Surg Res. 2015;193:519-522.
- Hartmann LC, Degnim AC, Santen RJ, et al. Atypical hyperplasia of the breast--risk assessment and management options. N Engl J Med. 2015;372(1):78-89.
- Hartmann LC, Radisky DC, Frost MH, et al. Understanding the premalignant potential of atypical hyperplasia through its natural history: a longitudinal cohort study. Cancer Prev Res. 2014;7(2):211-217.
- Sung JS, Malak SF, Bajaj P, et al. Screening breast MR imaging in women with a history of lobular carcinoma in situ. Radiology. 2011;261(2):414-420.
- Friedlander LC, Roth SO, Gavenonis SC. Results of MR imaging screening for breast cancer in high-risk patients with lobular carcinoma in situ. Radiology. 2011;261(2):421-427.
- King TA, Muhsen S, Patil S, et al. Is there a role for routine screening MRI in women with LCIS? Breast Cancer Res Treat. 2013;142(2):445-453.
- Mainiero MB, Lourenco A, Mahoney MC, et al. ACR Appropriateness Criteria Breast Cancer Screening. J Am Coll Radiol. 2013;10(1):11-14.
- Brennan S, Liberman L, Dershaw DD, Morris E. Breast MRI screening of women with a personal history of breast cancer. AJR Am J Roentgenol. 2010;195(2):510-516.
- Schacht DV, Yamaguchi K, Lai J, et al. Importance of a personal history of breast cancer as a risk factor for the development of subsequent breast cancer: results from screening breast MRI. AJR Am J Roentgenol. 2014;202(2):289-292.
- Antoniou AC, Casadei S, Heikkinen T, et al. Breast-cancer risk in families with mutations in PALB2. N Engl J Med. 2014;371(6):497-506.
- Kuhl CK, Schrading S, Strobel K, et al. Abbreviated breast magnetic resonance imaging (MRI): first postcontrast subtracted images and maximum-intensity projection-a novel approach to breast cancer screening with MRI. J Clin Oncol. 2014;32(22):2304-2310.





