Introduction
Liver-directed therapies for hepatic malignancies are used either in isolation [usually for hepatocellular carcinoma (HCC)] or in combination with systemic chemotherapy and/or surgery (for metastases or cholangiocarcinoma). Their role in the management of hepatic malignancies has progressed from being palliative in nature (hepatic artery–directed therapies) to curative with the introduction of ablative therapies and combination therapies (ablation plus hepatic artery–directed therapies). Additionally, these therapies form an integral part of hepatic transplantation for HCC by downsizing or controlling the tumor growth while patients await hepatic transplantation. In case of metastatic tumors, ablative therapy is often used as an adjunct to surgical resection, either to limit the extent of surgery or to treat bilobar disease. Despite the varied nature of these therapies, they all aim at providing minimally invasive therapy (as compared with surgery), minimizing the systemic effects of oncological therapy (as opposed to systemic chemotherapy), and minimizing the harmful effects on normal liver tissue while providing adequate tumor control. In addition, some of these therapies (eg, yttrium-90 [Y-90] radioembolization) appear to have a synergistic effect with systemic chemotherapy in achieving tumor control. We will discuss these therapeutic options in the management of HCC and hepatic metastases.
Hepatocellular Carcinoma
Curative therapies include hepatic transplantation, surgical resection, and ablation. Hepatic transplantation provides the best outcomes because it replaces the tumor and the cirrhotic liver that predisposes to subsequent tumors. Given the small number of available donor livers, defined criteria (eg, Milan, University of California, San Francisco) are used to select patients for optimal outcomes following hepatic transplantation.3,4 Surgical resection is reserved for the minority of patients presenting with early disease (3 nodules <3 cm each or 1 lesion <5 cm), no vascular invasion or extrahepatic spread, absence of portal hypertension, and good liver function (Child Pugh A status) and performance status (PS; ECOG PS 0). Ablation is considered a curative therapy for very early (single lesions <2 cm, Child-Pugh A status, and ECOG PS 0) and early-stage HCC, and is practiced in patients who are not eligible for surgical resection. Multifocal and bilobar tumors in asymptomatic patients with Child Pugh A/B status and good PS are managed with transarterial therapies. Advanced disease in patients presenting with symptoms, portal or hepatic venous invasion, and extrahepatic spread are triaged to either systemic therapy with sorafenib (Child Pugh A/B status and ECOG PS 1-2) or symptomatic therapy (Child Pugh C status and ECOG PS 3-4). However, a select group of such patients may potentially benefit from transarterial therapies, especially those with limited venous invasion and relatively preserved liver function and PS.2,5
The reported 5-year survival in the very early and early-stage HCC among those treated as per the BCLC algorithm is 50% to 70% compared with 20% in the untreated population.6 Chemoembolization improves survival in the intermediate stage of HCC, with reported median survival of 20 months compared with 16 months in the untreated population. In the advanced stage, sorafenib therapy is associated with improved median survival (10.7 months vs 7.9 months).7 Transarterial therapy in a select group of patients with advanced stage improved median survival (13.3 months).5 Outcomes in the terminal stage HCC are poor (<3 months).6
Ablative Therapies
In RFA, a high frequency alternating current (450–500 kHz) is passed through an electrode (the probe that is placed into the tumor). This results in frictional heat (50 degrees C-105 degrees C) generation, and the heat is conducted into the surrounding tumor cells, leading to coagulative necrosis and cell death. Radiofrequency ablation is widely available, extensively studied, and is an established treatment modality. The main limitations of RFA relate to decreased or nonuniform heat distribution resulting in higher local recurrence rates in the presence of adjacent high-flow blood vessels (“heat sink effect”) and from charring/dessication around the probe.10 Microwave ablation uses electromagnetic waves that result in the vibration of water molecules within the tissue, leading to heat generation and cellular death. Microwave ablation is less time-consuming compared with RFA, and allows for excellent uniform heat distribution without any heat sink from adjacent vessels. Despite the theoretical benefits of MWA, studies report similar outcomes compared with RFA.11 Freezing from rapid expansion of gas through a low-pressure probe in combination with thawing cycles during cryoablation results in intracellular dehydration and cell death. Cryoablation is well suited for ablation of tumors that are in proximity to vital structures, and offers the ability for real-time monitoring of the treatment zone. However, cryoablation carries the risks of hemorrhage (<2%) and cryoshock (2%), especially in patients with underlying cirrhosis and coagulopathy.12,13 Other ablative therapies such as laser and high-intensity focused ultrasound are of limited proven utility in the treatment of HCC lesions, but may have an added benefit when combined with other therapies.14 Ablation is recommended for very early and early-stage HCC as an alternative to surgical resection, and for downstaging/bridging considerations of intermediate-stage HCC prior to hepatic transplantation.15,16 Despite conflicting data, ablation for very early and early-stage HCC is considered to be as effective as surgical resection with similar survival outcomes.17-20 An ideal lesion for ablation is a small (<3 cm), peripheral, noncapsular HCC that is distant from the vital structures (gall bladder, common bile duct, diaphragm, and pericardium) and vasculature. Multiple lesions can be ablated, but procedure times and technical issues limit its use for up to three lesions during one treatment session. Tumors larger than 3 cm are routinely triaged to other regional therapies due to the risk of local recurrence with RFA. However, MWA, which allows synchronized tumor ablation with multiple probes and combination of RFA, and chemical ablation allow treatment of larger tumors (up to 5 cm) with great success.21,22 Additionally, larger tumors can be successfully treated with a combination of RFA and chemoembolization.23-25 The sequence of these procedures is not standardized, but the authors of this article typically practice chemoembolization first, followed by ablation. This approach has two advantages: (1) the tumor can be successfully “stained” with lipiodol during transarterial chemoembolization (TACE) that allows visualization of the tumor on noncontrast computed tomography (CT) for easy targeting during ablation; and (2) embolization decreases the risk of heat sink effect. Laparoscopic ablation is useful for lesions adjacent to the pericardium and the dome of the diaphragm, although the latter could be approached percutaneously though a transpleural route by creating an artificial pneumothorax.26 Ablative therapies are safe, but risks include pain (for lesions adjacent to the diaphragm or abdominal wall), bleeding, and injury to adjacent vital structures such as the biliary system.27 The results of ablation for HCC are summarized in Table 1.

Transarterial Therapies
Transarterial therapies take advantage of differential blood supply of the tumors (supplied by the hepatic artery) and normal liver parenchyma (predominantly supplied by the portal vein), and high microvessel density within the tumors resulting from tumoral angiogenesis. The commonly applied transarterial therapies involve various microembolic materials, and include particle embolization without any chemotherapy (also called transarterial embolization [TAE] or bland embolization), chemoembolization with lipiodolchemotherapy emulsion and microparticles or gel foam (conventional chemoembolization [cTACE]), chemoembolization with drug-eluting microspheres (DEB-TACE), and Y-90 microsphere radioembolization. These therapies result in tumor ischemia, and the level of arteriolar/precapillary occlusion is dependent on the size of the beads. Given the ischemic effects, these therapies are associated with postembolic syndrome manifested by fever, pain, malaise, fatigue, and mild to moderate alterations in liver function tests. These symptoms most often are associated with TAE, cTACE, and DEB-TACE, and less commonly with Y-90.
Transarterial Embolization
Chemoembolization

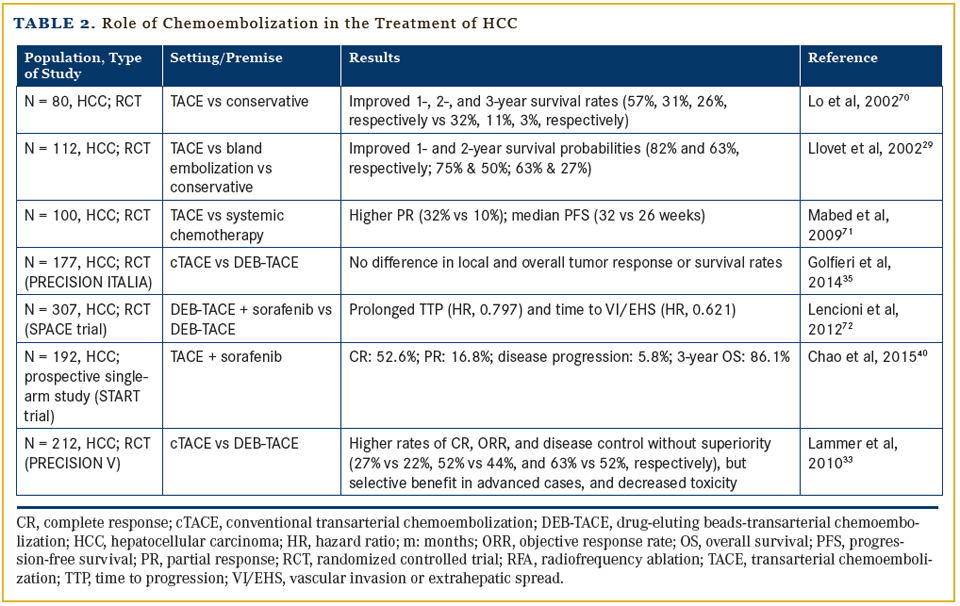
The overall survival (OS) following chemoembolization is dependent on underlying liver disease, tumor burden, intravenous extension of the tumor, and extrahepatic metastases.36 The number of chemoembolization procedures and tumor response following chemoembolization are associated with superior survival.5,36,37 Recent reports suggest that DEB-TACE is safe and improves survival in patients with advanced HCC (BCLC C stage), especially in those with minimal symptoms, limited portal venous invasion, preserved liver function, and ECOG PS ≤1.5,38 Initial reports from a recent study investigating the role of concurrent sorafenib therapy during chemoembolization suggests no significant increase in toxicity, but survival benefits are unknown.39,40 Results of chemoembolization are listed in Table 2. Most patients develop self-limiting postembolization syndrome (nausea, pain, fever) following chemoembolization. Complications of chemoembolization include liver failure (<5%); bone marrow suppression, renal failure, cardiac toxicity, abscess (<3%); and cholecystitis (<1%).41 Bilio-enteric anastomosis, advanced liver disease, and prior chemotherapy increase the risk of postprocedure complications. In general, DEB-TACE has a superior safety profile compared with cTACE.34
Radioembolization
Given that the size of Y-90 particles (20 μm-60 μm ) is much smaller than those applied for chemoembolization and high toxicity associated with beta radiation, additional precautions are necessary during Y-90 therapy. A planning angiogram is performed to identify and occlude extrahepatic branches of the hepatic artery that might potentially lead to nontarget Y-90 distribution. Additionally, technitium-99m-labeled macro-aggregated albumin particles are intra-arterially administered to assess intra-hepatic particle distribution, and to calculate hepatopulmonary shunt that results from intratumoral arteriovenous communications. Subsequently, the Y-90 dose is calculated based on the tumor-to-liver ratio and lung shunt fraction, and is administered in the lobar or segmental arteries. High lung shunting (which can lead to radiation pneumonitis), extensive extrahepatic metastatic disease, severe liver dysfunction, and difficult anatomy with uncorrectable nontarget distribution preclude Y-90 therapy.
A study by Salem et al42 reported longer time to progression following Y-90 without significant change in OS when compared with cTACE and DEB-TACE. However, Y-90 was associated with less postembolic syndrome compared with cTACE/DEB-TACE, and was reported to be more cost-effective in a select group of patients.42,44,45 In addition, Y-90 may be better tolerated in patients with intravenous tumor invasion. The comparative roles of Y-90 versus chemoembolization (PREMIERE trial46) and Y-90 versus sorafenib in advanced HCC (SARAH trial47) are being investigated. Postembolization syndrome following Y-90 occurs in 20% to 50% of patients. Complications of Y-90 therapy include Y-90 bowel injury (<5%), radiation pneumonitis (<1%), liver failure (0%-4%), biliary complications (<10%), radiation dermatitis, and bone marrow suppression.48,49 The results of Y-90 treatment are listed in Table 3.

Cholangiocarcinoma
Hepatic Metastases
The recent randomized studies comparing FOLFOX versus FOLFOX plus SIR-Spheres (SIRFLOX57 and FOXFIRE58) demonstrated superior progression-free survival (PFS) with the latter, but no significant improvement in OS of patients with colorectal hepatic metastases. The role of DEBIRI is still evolving and appears to be effective in improving both PFS and OS.59 The results of DEBIRI and radioembolization for hepatic metastases are listed in Table 4.

Hepatic metastases from neuroendocrine tumors are often indolent, but can be symptomatic from hormone secretion, capsular stretching, and tumor burden. Transarterial bland embolization, chemoembolization, and radioembolization have been applied for locoregional control of the disease when surgery is not an option.60 No randomized trials exist comparing various transarterial therapies. The outcomes of various transarterial therapies are similar with reported 1-, 2-, 3-, and 5-year survival of 85%, 63%, 46%, 50% with Y-90, respectively, and 75% , 66%, 48%, and 37% with TACE/TAE treatments, respectively.61 Uveal melanoma has a high propensity for liver metastases despite successful treatment of the primary tumor. The prognosis is poor, and systemic therapy is relatively ineffective in the presence of hepatic metastatic disease. Locoregional therapy with hepatic arterial infusion, immunoembolization, chemoembolization, and radioembolization provide local control of hepatic disease and prolong survival. Median survival following Y-90 therapy ranges from 7 months to 10 months.62,63
Conclusion
Affiliations: Murthy R. Chamarthy, MD, and Sanjeeva P. Kalva, MD, are from the University of Texas Southwestern Medical Center, Dallas.
Disclosures: None
Address correspondence to: Sanjeeva P. Kalva MD, Interventional Radiology, University of Texas Southwestern Medical Center, Dallas, TX 75390-8834; email: Sanjeeva.Kalva @UTSouthwestern.edu
References
- Child CG, Turcotte JG. Surgery and portal hypertension.Major Probl Clin Surg. 1964;1:1-85.
- Llovet JM, Fuster J, Bruix J, Barcelona-Clinic Liver Cancer G. The Barcelona approach: diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl. 2004;10(2 Suppl 1):S115-120.
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693-699.
- Yao FY, Ferrell L, Bass NM, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33(6):1394-1403.
- Kalva SP, Pectasides M, Liu R, et al. Safety and effectiveness of chemoembolization with drug-eluting beads for advanced-stage hepatocellular carcinoma [published online June 12, 2013]. Cardiovasc Intervent Radiol. 2014;37(2):381-387. doi: 10.1007/ s00270-013-0654-7.
- Llovet JM, Di Bisceglie AM, Bruix J, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst. 2008;100(10):698-711.
- Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378-390.
- Ebara M, Okabe S, Kita K, et al. Percutaneous ethanol injection for small hepatocellular carcinoma: therapeutic efficacy based on 20-year observation. J Hepatol. 2005;43(3):458-464.
- Yin XY, Lu MD. Percutaneous ablation for small hepatocellular carcinoma. Expert Rev Gastroenterol Hepatol. 2009;3(2):121-130.
- Goldberg SN, Hahn PF, Tanabe KK, et al. Percutaneous radiofrequency tissue ablation: does perfusion-mediated tissue cooling limit coagulation necrosis? J Vasc Interv Radiol. 1998; 9(1 Pt 1):101-111.
- Vogl TJ, Farshid P, Naguib NN, et al. Ablation therapy of hepatocellular carcinoma: a comparative study between radiofrequency and microwave ablation. Abdom Imaging. 2015;40(6):1829-1837.
- Niu LZ, Li JL, Xu KC. Percutaneous cryoablation for liver cancer. J Clin Transl Hepatol. 2014;2(3):182-188.
- Rong G, Bai W, Dong Z, et al. Long-term outcomes of percutaneous cryoablation for patients with hepatocellular carcinoma within Milan criteria. PLoS One. 2015;10(4):e0123065.
- Kim J, Chung DJ, Jung SE, et al. Therapeutic effect of high-intensity focused ultrasound combined with transarterial chemoembolisation for hepatocellular carcinoma <5 cm: comparison with transarterial chemoembolisation monotherapy--preliminary observations. Br J Radiol. 2012;85(1018):e940-946.
- Shiina S, Tateishi R, Arano T, et al. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am J Gastroenterol. 2012;107(4):569-577; quiz 578.
-
Mazzaferro V, Battiston C, Perrone S, et al. Radiofrequency ablation of small hepatocellular carcinoma in cirrhotic patients
awaiting liver transplantation: a prospective study. Ann Surg. 2004;240(5):900-909. -
Weis S, Franke A, Mossner J, et al. Radiofrequency (thermal) ablation versus no intervention or other interventions
for hepatocellular carcinoma. Cochrane Database Syst Rev. 2013;12:CD003046. - Duan C, Liu M, Zhang Z, et al. Radiofrequency ablation versus hepatic resection for the treatment of early-stage hepatocellular carcinoma meeting Milan criteria: a systematic review and meta-analysis. World J Surg Oncol. 2013;11(1):190.
- Peng ZW, Liu FR, Ye S, et al. Radiofrequency ablation versus open hepatic resection for elderly patients (> 65 years) with very early or early hepatocellular carcinoma. Cancer. 2013;119(21):3812-3820.
-
Zhou Y, Zhao Y, Li B, et al. Meta-analysis of radiofrequency ablation versus hepatic resection for small hepatocellular
carcinoma. BMC Gastroenterol. 2010;10:78. -
Lin JW, Lin CC, Chen WT, Lin SM. Combining radiofrequency ablation and ethanol injection may achieve comparable long-term outcomes in larger hepatocellular carcinoma (3.1-4 cm) and in high-risk locations. Kaohsiung J Med
Sci. 2014;30(8):396-401. - Vallone P, Catalano O, Izzo F, Siani A. Combined ethanol injection therapy and radiofrequency ablation therapy in percutaneous treatment of hepatocellular carcinoma larger than 4cm. Cardiovasc Intervent Radiol. 2006;29(4):544-551.
- Veltri A, Moretto P, Doriguzzi A, et al. Radiofrequency thermal ablation (RFA) after transarterial chemoembolization (TACE) as a combined therapy for unresectable non-early hepatocellular carcinoma (HCC). Eur Radiol. 2006;16(3):661-669
- Lu Z, Wen F, Guo Q, et al. Radiofrequency ablation plus chemoembolization versus radiofrequency ablation alone for hepatocellular carcinoma: a meta-analysis of randomized-controlled trials. Eur J Gastroenterol Hepatol. 2013;25(2):187-194.
- Bonomo G, Della Vigna P, Monfardini L, et al. Combined therapies for the treatment of technically unresectable liver malignancies: bland embolization and radiofrequency thermal ablation within the same session. Cardiovasc Intervent Radiol. 2012;35(6):1372-1379.
- El-Gendi A, El-Shafei M, Abdel-Aziz F, Bedewy E. Intraoperative ablation for small HCC not amenable for percutaneous radiofrequency ablation in Child A cirrhotic patients. J Gastrointest Surg. 2013;17(4):712-718.
- Kong WT, Zhang WW, Qiu YD, et al. Major complications after radiofrequency ablation for liver tumors: analysis of 255 patients. World J Gastroenterol. 2009;15(21):2651-2656.
- Malagari K, Pomoni M, Kelekis A, et al. Prospective randomized comparison of chemoembolization with doxorubicin-eluting beads and bland embolization with BeadBlock for hepatocellular carcinoma. Cardiovasc Intervent Radiol. 2010;33(3):541-551.
- Llovet JM, Real MI, Montana X, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002;359(9319):1734-1739.
- Meyer T, Kirkwood A, Roughton M, et al. A randomised phase II/III trial of 3-weekly cisplatin-based sequential transarterial chemoembolisation vs embolisation alone for hepatocellular carcinoma. Br J Cancer. 2013;108(6):1252-1259.
- Brown KT, Gonen M, Do KG, et al. A randomized single blind controlled trial of beads versus doxorubicin-eluting beads for arterial embolization of hepatocellular carcinoma (HCC). J Clin Oncol. 2013;31:143.
- Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology. 2003;37(2):429-442.
-
Lammer J, Malagari K, Vogl T, et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study.
Cardiovasc Intervent Radiol. 2010;33(1):41-52. - Vogl TJ, Lammer J, Lencioni R, et al. Liver, gastrointestinal, and cardiac toxicity in intermediate hepatocellular carcinoma treated with PRECISION TACE with drug-eluting beads: results from the PRECISION V randomized trial. AJR Am J Roentgenol. 2011;197(4):W562-570.
- Golfieri R, Giampalma E, Renzulli M, et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellularcarcinoma. Br J Cancer. 2014;111(2):255-264.
- Kalva SP, Pectasides M, Yeddula K, et al. Factors affecting survival following chemoembolization with doxorubicin-eluting microspheres for inoperable hepatocellular carcinoma. J Vasc Interv Radiol. 2013;24(2):257-265.
- Georgiades C, Geschwind JF, Harrison N, et al. Lack of response after initial chemoembolization for hepatocellular carcinoma: does it predict failure of subsequent treatment? Radiology. 2012;265(1):115-123.
- Ray CE, Jr., Brown AC, Green TJ, et al. Survival outcomes in patients with advanced hepatocellular carcinoma treated with drug-eluting bead chemoembolization. AJR Am J Roentgenol. 2015;204(2):440-447.
- Cosgrove DP, Reyes DK, Pawlik TM, et al. Open-label single-arm phase II trial of sorafenib therapy with drug-eluting bead transarterial chemoembolization in patients with unresectable hepatocellular carcinoma: clinical results. Radiology. 2015;277(2):594-603.
- Chao Y, Chung YH, Han G, et al. The combination of transcatheter arterial chemoembolization and sorafenib is well tolerated and effective in Asian patients with hepatocellular carcinoma: final results of the START trial. Int J Cancer. 2015;136(6):1458-1467.
- Clark TW. Complications of hepatic chemoembolization. Semin Intervent Radiol. 2006;23(2):119-125.
- Salem R, Lewandowski RJ, Kulik L, et al. Radioembolization results in longer time-to-progression and reduced toxicity compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2011;140(2):497-507e2.
-
Riaz A, Gates VL, Atassi B, et al. Radiation segmentectomy: a novel approach to increase safety and efficacy of radioembolization. Int J Radiat Oncol Biol Phys. 2011;79(1):163-
171. -
Ray CE, Jr., Battaglia C, Libby AM, et al. Interventional radiologic treatment of hepatocellular carcinoma-a cost analysis from the payer perspective. J Vasc Interv Radiol. 2012;23(3):306-
314. - Rostambeigi N, Dekarske AS, Austin EE, et al. Cost effectiveness of radioembolization compared with conventional transarterial chemoembolization for treatment of hepatocellular carcinoma. J Vasc Interv Radiol. 2014;25(7):1075-1084.
- Vilgrain V, Abdel-Rehim M, Sibert A, et al. Radioembolisation with yttrium90 microspheres versus sorafenib for treatment of advanced hepatocellular carcinoma (SARAH): study protocol for a randomised controlled trial. Trials. 2014;15:474.
- ClinicalTrials.gov. Identifier NCT00956930. Chemoembolization versus radioembolization in treating patients with liver cancer that cannot be treated with radiofrequency ablation or surgery. https://clinicaltrials.gov/ ct2/show/NCT00956930. Accessed December 17, 2015.
- Salem R, Lewandowski RJ, Atassi B, et al. Treatment of unresectable hepatocellular carcinoma with use of 90Y microspheres (TheraSphere): safety, tumor response, and survival. J Vasc Interv Radiol. 2005;16(12):1627-1639.
- Riaz A, Awais R, Salem R. Side effects of yttrium-90 radioembolization. Front Oncol. 2014;4:198.
- Kuhlmann JB, Blum HE. Locoregional therapy for cholangiocarcinoma. Curr Opin Gastroenterol. 2013;29:324-328.
- Hyder O, Marsh JW, Salem R, et al. Intra-arterial therapy for advanced intrahepatic cholangiocarcinoma: a multi-institutional analysis. Ann Surg Oncol. 2013;20(12):3779-3786.
- Boehm LM, Jayakrishnan TT, Miura JT, et al. Comparative effectiveness of hepatic artery based therapies for unresectable intrahepatic cholangiocarcinoma. J Surg Oncol. 2015;111(2):213-220.
- Siperstein AE, Berber E, Ballem N, Parikh RT. Survival after radiofrequency ablation of colorectal liver metastases: 10-year experience. Ann Surg. 2007;246(4):559-565; discussion 565-567.
- Kennedy AS, Coldwell D, Nutting C, et al. Resin 90Y-microsphere brachytherapy for unresectable colorectal liver metastases: modern USA experience. Int J Radiat Oncol Biol Phys. 2006;65(2):412-425.
- Kalva SP, Rana RS, Liu R, et al. Yttrium-90 radioembolization as salvage therapy for liver metastases from colorectal cancer [published online November 4, 2014]. Am J Clin Oncol. 2014.
-
Saxena A, Bester L, Shan L, et al. A systematic review on the safety and efficacy of yttrium-90 radioembolization for unresectable, chemorefractory colorectal cancer liver metastases.
J Cancer Res Clin Oncol. 2014;140(4):537-547. - Gibbs P, Gebski V, Van Buskirk M, et al. Selective Internal Radiation Therapy (SIRT) with yttrium-90 resin microspheres plus standard systemic chemotherapy regimen of FOLFOX versus FOLFOX alone as first-line treatment of non-resectable liver metastases from colorectal cancer: the SIRFLOX study. BMC Cancer. 2014;14:897.
- Dutton SJ, Kenealy N, Love SB, et al. FOXFIRE protocol: an open-label, randomised, phase III trial of 5-fluorouracil, oxaliplatin and folinic acid (OxMdG) with or without interventional Selective Internal Radiation Therapy (SIRT) as first-line treatment for patients with unresectable liver-only or liver-dominant metastatic colorectal cancer. BMC Cancer. 2014;14:497.
- Fiorentini G, Aliberti C, Tilli M, et al. Intra-arterial infusion of irinotecan-loaded drug-eluting beads (DEBIRI) versus intravenous therapy (FOLFIRI) for hepatic metastases from colorectal cancer: final results of a phase III study. Anticancer Res. 2012;32(4):1387-1395.
- Grandhi MS, Lafaro KJ, Pawlik TM. Role of locoregional and systemic approaches for the treatment of patients with metastatic neuroendocrine tumors. J Gastrointest Surg. 2015;19(12):2273-2282.
- Yang TX, Chua TC, Morris DL. Radioembolization and chemoembolization for unresectable neuroendocrine liver metastases - a systematic review. Surg Oncol. 2012;21(4):299-308.
- Eschelman DJ, Gonsalves CF, Sato T. Transhepatic therapies for metastatic uveal melanoma. Semin Intervent Radiol. 2013;30(1):39-48.
-
Klingenstein A, Haug AR, Zech CJ, Schaller UC. Radioembolization as locoregional therapy of hepatic metastases in uveal melanoma patients. Cardiovasc Intervent Radiol.
2013;36(1):158-165. - Chen MS, Li JQ, Zheng Y, et al. A prospective randomized trial comparing percutaneous local ablative therapy and partial hepatectomy for small hepatocellular carcinoma. Ann Surg. 2006;243(3):321-328.
- Lu MD, Kuang M, Liang LJ, et al. [Surgical resection versus percutaneous thermal ablation for early-stage hepatocellular carcinoma: a randomized clinical trial]. Zhonghua Yi Xue Za Zhi. 2006;86(12):801-805.
- Shiina S, Teratani T, Obi S, et al. A randomized controlled trial of radiofrequency ablation with ethanol injection for small hepatocellular carcinoma. Gastroenterology. 2005;129(1):122-130.
- Kagawa T, Koizumi J, Kojima S, et al. Transcatheter arterial chemoembolization plus radiofrequency ablation therapy for early stage hepatocellular carcinoma: comparison with surgical resection. Cancer. 2010;116(15):3638-3644.
- Wang C, Wang H, Yang W, et al. Multicenter randomized controlled trial of percutaneous cryoablation versus radiofrequency ablation in hepatocellular carcinoma. Hepatology. 2015;61(5):1579-1590.
- Shi J, Sun Q, Wang Y, et al. Comparison of microwave ablation and surgical resection for treatment of hepatocellular carcinomas conforming to Milan criteria. J Gastroenterol Hepatol. 2014;29(7):1500-1507.
- Lo CM, Ngan H, Tso WK, et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology. 2002;35(5):1164-1171.
- Mabed M, Esmaeel M, El-Khodary T, et al. A randomized controlled trial of transcatheter arterial chemoembolization with lipiodol, doxorubicin and cisplatin versus intravenous doxorubicin for patients with unresectable hepatocellular carcinoma. Eur J Cancer Care (Engl). 2009;18(5):492-499.
- Lencioni R LJ, Han G, et al. Sorafenib or placebo in combination with transarterial chemoembolization (TACE) with doxorubicin-eluting beads (DEBDOX) for intermediate-stage hepatocellular carcinoma (HCC): phase II, randomized, double-blind SPACE trial. J Clin Oncol. 2012;30 (suppl 4; abstr LBA154).
- Salem R, Lewandowski RJ, Mulcahy MF, et al. Radioembolization for hepatocellular carcinoma using Yttrium-90 microspheres: a comprehensive report of long-term outcomes. Gastroenterology. 2010;138(1):52-64.
- Carr BI, Kondragunta V, Buch SC, Branch RA. Therapeutic equivalence in survival for hepatic arterial chemoembolization and yttrium 90 microsphere treatments in unresectable hepatocellular carcinoma: a two-cohort study. Cancer. 2010;116(5):1305-1314.
- Lewandowski RJ, Kulik LM, Riaz A, et al. A comparative analysis of transarterial downstaging for hepatocellular carcinoma: chemoembolization versus radioembolization. Am J Transplant. 2009;9(8):1920-1928.
- Rosenbaum CE, Verkooijen HM, Lam MG, et al. Radioembolization for treatment of salvage patients with colorectal cancer liver metastases: a systematic review. J Nucl Cardiol. 2013;54(11):1890-1895.





